


Streamlining Prior Authorization with Generative AI
Part of the `AI That Matters` Series 🌟


By Pablo Salvador Lopez & Shiva Pedram, M.D.
December 19, 2024
🗐 This article is for educational purposes only. The scenarios (data) are fictional, and no real patient data is used. It aims to demonstrate AI's potential in healthcare.
The Future of Prior Authorization
Imagine having a colleague who scans policies faster than a seasoned compliance officer, extracts key details with the precision of a surgeon, and cross-checks documentation with endless patience. It’s not magic — it’s AI. But not just any AI — it’s an AI that understands the burden of prior authorization and tackles it head-on, so you can focus on decisions, not paperwork.
I have created a project that does just that, and its name is AutoAuth. No, it's not here to replace you; it's here to amplify you.
AutoAuth in Action
To clarify, this is not a product—it's a code-first modular approach. We built a UI layer to easily showcase the power of the AutoAuth framework to process prior authorization (PA) ! You have access to the code and customize as needed.
What is this article about?
This article introduces AutoAuth, an AI-driven solution with the potential to transform prior authorization workflows. By automating policy searches, document extraction, and cross-checks, AutoAuth allows healthcare professionals to focus on decisions, not busywork. Whether you're a leader looking for impact or a developer seeking technical depth, this article provides both. — clear strategy and practical execution.
What is Prior Authorization (PA) ?
PA is a process that requires healthcare providers to obtain approval from insurance companies before certain medications, treatments, or procedures can be covered. While designed to manage costs and ensure the appropriateness of care, the process often creates friction between payers and providers, leading to delays in necessary treatment and increased frustration.
The Problem: Studies have shown that the PA process can lead to treatment delays, with 93% of physicians reporting that PA’s delay access to necessary care, leading to treatment abandonment in 82% of cases [1]. Patients sometimes experience worsened health outcomes due to the time lost in approval back-and-forths. Even a one-week delay in critical treatments such as cancer, increases mortality risk by 1.2–3.2% [3].
Impact on Patients & Providers: Physicians handle an average of 41 PA requests per week, consuming around 13 hours, equivalent to two business days [1]. For the payers who process these requests, up to 75% of PA tasks are manual or partially manual, resulting in high cost burdens per transaction [2]. In addition, the failure to provide timely PA decisions “can literally mean life or death for patients,” as physicians have reported in surveys, “when care is urgent, 72 hours is simply not a safe amount of time to wait to receive approval for coverage [11].”
The Solution - Automation with AutoAuth: Automation presents a promising solution, enabling more efficient communication between payers and providers, reducing manual administrative tasks, and accelerating decision-making. By implementing automated systems to handle the prior authorization process, stakeholders can reduce delays, cut costs, and free up resources to focus on what truly matters: optimizing patient care and ensuring timely access to essential medications and treatments [2][3].
AutoAuth at a Glance
AI-driven end-to-end PA automation
Accelerates decisions from days to minutes, expediting patient care
It is not a product; it is a framework. Purpose-built to tackle the complexities of prior authorization, it could integrate seamlessly with both payor and provider systems. With a modular, code-first architecture and a flexible, loosely coupled design, it ensures adaptability and scalability. Built on the Azure cloud, it enables seamless customization to meet the unique needs of complex and despair PA workflows.
Significant cost and labor reductions for both payers and providers
Overview of Today's Prior Authorization Workflow

On the left, providers—represented by pharmacists, nurses, and physicians—gather and process patient data from multiple sources such as Electronic Health Records (EHR), Laboratory Information Systems (LIS), Picture Archiving and Communication Systems (PACS), Clinical Decision Support Systems (CDSS), and finance databases
This data, both structured and unstructured, undergoes a rigorous intake and processing phase before PA submission
The payers’ side then takes over, where administrative staff review clinical information, route data, analyze coverage, and make eligibility determinations primarily through unstructured means like fax and portal submissions
The Pain Points
Time delays: The process for approval decisions can take anywhere from hours to weeks, depending on the case.
Provider burden: 13 hours per week are spent on PAs, with a heavy reliance on human intervention on both sides. Prone to human error due to volume.
Patient outcomes: Delays in authorization often affect important care schedules, such as cancer treatment.
Cost to System: High costs per transaction arise due to the time and human effort needed for processing.
The Turning Point for AI in Prior Authorization
Systemic Burden + Regulatory Overhaul + Explosive Technological Advancements = A Defining Moment for Innovation
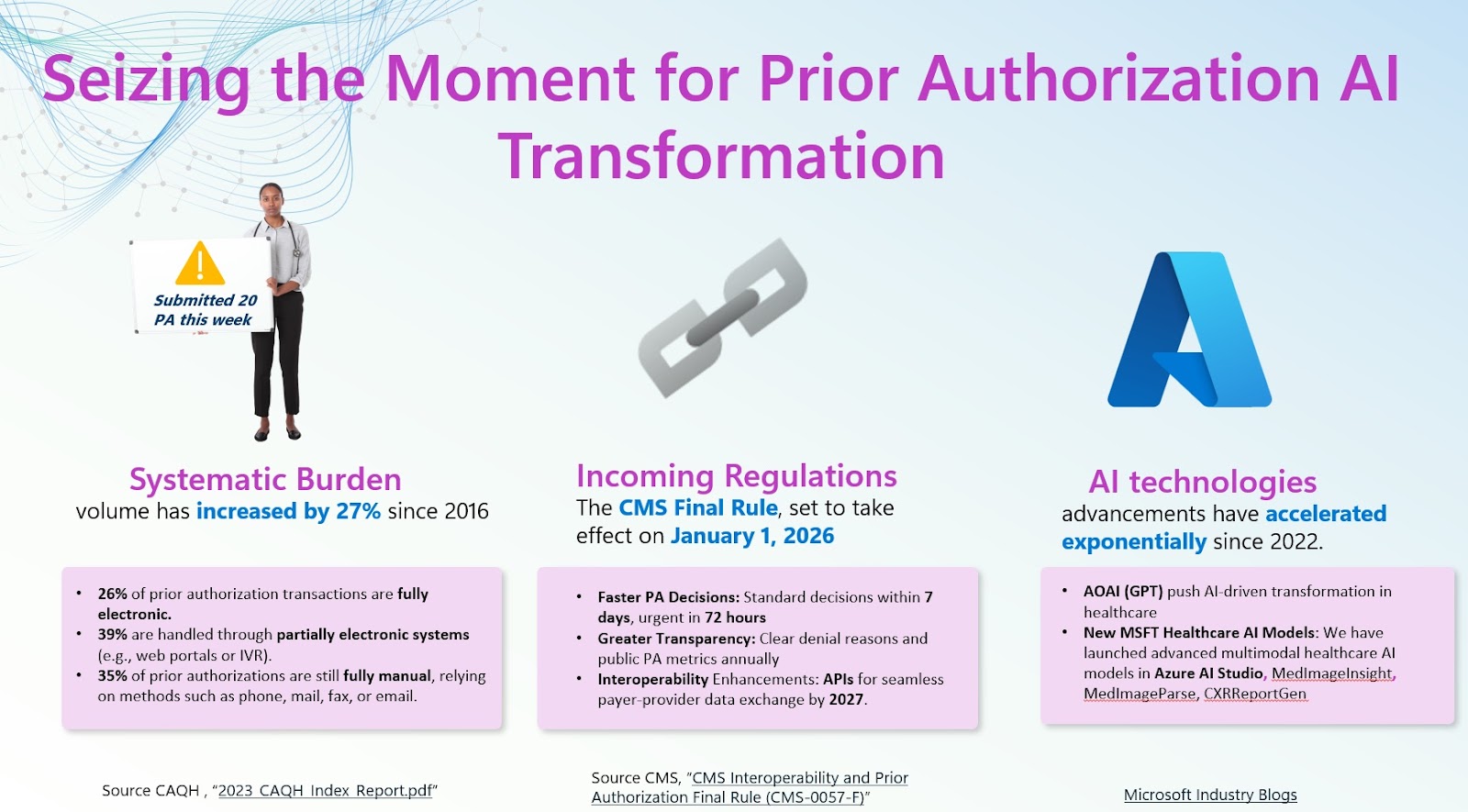
Regulatory Change: On January 17 of 2024, the Centers for Medicare and Medicaid Services (CMS) issued a Final Rule (CMS-0057-F), a new requirement mandating payers to process PA’s within 72 hours for urgent requests and within 7 days for standard requests in an effort to promote efficiency. It was also mandated that payers will need to issue detailed reasoning for denials, in an effort to improve communication and transparency. These requirements must be implemented beginning January 1, 2026, and by 2027 payers must implement and maintain an API (application programming interface) [4]. The 2023 CAQH Index Report also indicates a 23% increase in medical transaction volumes, with electronic prior authorizations surging by 61%. This surge has led to a 30% rise in spending on prior authorizations, amounting to an additional $1.3 billion compared to the previous year. Thus, not only do prior authorization requests need to be processed faster by 2026, but these requirements are emerging in the face of ever-increasing volumes and costs of PA requests, creating an urgent need for reformation of the PA process [5].
Automation Needed to Meet Today's and Tomorrow's Demands:
Faster decision-making (minutes, not days)
Reduced administrative load
Improved transparency and clarity on approvals/denials
Direct compliance with the CMS Final Rule (CMS-0057-F)
AutoAuth Methodology
The purpose of AutoAuth is to act as a supportive recommendation system for policy decisions. We will demonstrate how AutoAuth is able to analyze, extract, and interpret clinical information including: physician documentation, laboratory results, imaging results, pathology reports, and PA submission forms all while retrieving and cross-referencing the relevant PA insurance policy in order to approve or deny the requested medication with detailed reasoning.
Holistic Workflow Overview
The system is designed around four key phases:
Knowledge Base Construction: Builds a centralized repository of policies and guidelines for efficient retrieval.
Unstructured Clinical Data Processing: Extracts, normalizes, and structures key information from clinical documents.
Agentic RAG - Intelligent Policy Matching: Uses agent-driven retrieval to match clinical data with the most relevant policy.
Claims Processing: Automates claim evaluations and provides decision support for approvals or denials.

Phase 1: Knowledge Base Construction
Objective: Establish a centralized repository of Prior Authorization (PA) policies and guidelines to streamline the decision-making process.
Workflow:
Policy Ingestion:
Sources: Gather policy documents from diverse origins, including PDFs, Word files, and scanned images.
Approach: Utilize advanced Optical Character Recognition (OCR) integrated with Document Intelligence to extract text from these documents.
Indexing:
- Storage: Implement Azure AI Search to store the data, leveraging its semantic embedding capabilities for efficient and precise retrieval, facilitating context-aware information retrieval.
Key Technologies and Implementation Insights:
Optical Character Recognition (OCR) extracts text from unstructured documents, enabling digital analysis, while Azure AI Search powers semantic and lexical search for precise data retrieval. Embedding models further enhance this process by capturing semantic relationships within the data. To construct the knowledge base, we used publicly available PA policies in PDF format were ingested and processed. By integrating Azure AI Search's vector search and semantic ranking capabilities, the system enables advanced, context-aware retrieval of relevant policies, ensuring more accurate and efficient search results.
Phase 2: Unstructured Clinical Data Processing
Objective: Extract and structure patient-specific clinical information from raw data sources using advanced Large Language Model (LLM)-based techniques.
Workflow:
Data Aggregation
- Sources: Collect unstructured clinical data from Electronic Health Records (EHRs), Laboratory Information Systems (LIS), Picture Archiving and Communication Systems (PACS), and scanned provider documents.
LLM-Based Data Extraction
Natural Language Processing (NLP): Use LLMs to analyze unstructured text and identify key clinical entities.
Entity Recognition: Extract and classify critical data points, including:
Patient demographics (e.g., name, date of birth, contact details)
Diagnoses (e.g., ICD-10 codes)
Treatment plans
Laboratory results and imaging findings
Disambiguation: Address ambiguities in medical terminology to ensure accurate and consistent data extraction.
Data Structuring
- Standardization: Convert extracted information into structured formats (e.g., JSON) to enable smooth integration with downstream systems and applications.
Key Technologies and Implementation Insights:
Phase 3: Agentic RAG - Intelligent Policy Matching
Objective:
Identify the most relevant PA policy for a clinical case using a multi-layered retrieval approach, supported by Azure AI Search and LLM as the formulator and judge.
Workflow:
Query Generation: Construct precise and context-rich queries from structured clinical data, capturing all essential attributes of the patient's case.
Retrieval: Use either BM25 or semantic search based on the query type, or combine both with hybrid retrieval for best results.
Semantic Search: Retrieve policies based on contextual similarity using vector embeddings. Leverage the capabilities of Azure AI Search to enhance retrieval precision in a single API call.
Hybrid Retrieval + L2 Ranking:
Layer 1 (L1 - Retrieval): Conducts the initial retrieval using a mix of semantic (vector-based) and lexical (keyword-based) methods. Results from both are combined using Reciprocal Rank Fusion (RRF), balancing the strengths of each method.
Layer 2 (L2 - Semantic Ranking): Refines the top results from L1 using a transformer-based model, adjusting scores based on deeper contextual alignment between the query and documents. This ensures the most contextually relevant policies are ranked highest.
Keyword Search (BM25): Match keywords and phrases for precision. LLM as Judge..The LLM acts as an evaluator, assessing the second layer of subjectivity to determine whether the predicted relevant policies retrieved from the coverage knowledge store align with the policy criteria and the clinical details required to make a determination.
Retrieval Evaluator: The LLM acts as an evaluator, assessing the second layer of subjectivity to determine whether the predicted relevant policies retrieved from the coverage knowledge store align with the policy criteria and the clinical details required to make a determination.
Key Technologies and Implementation Insights:
Phase 4: Claims Processing
Objective: Cross-reference patient, physician, and clinical details against policy criteria. Classify the Prior Authorization (PA) claim as Approved, Denied, or Needs More Information, providing clear, evidence-based explanations and policy references to support a comprehensive human final determination.
Workflow:
Policy Criteria Evaluation:
Assess each policy criterion against the structured clinical data.
Mark as Fully Met, Partially Met, or Not Met based on alignment with policy guidelines.
Gap Identification:
Identify missing or incomplete information required to complete the evaluation.
Request additional details if critical gaps are found.
Recommendation Generation:
Approval: All policy criteria are fully satisfied.
* Denial: One or more policy criteria are not met.
* Needs More Information: Critical data is missing for evaluation.
Key Technologies and Implementation Insights:
The recommendation engine leverages a combination of advanced technologies to ensure precision and transparency in evaluating PA requests. At its core, chained reasoning provides a step-by-step logical framework to systematically assess multi-step policy criteria, ensuring no detail is overlooked. Complementing this, LLMs (GPT-o1 Series) bring advanced reasoning capabilities to the process. These models synthesize patient data and policy requirements, cross-referencing clinical documents with policy text to generate precise and comprehensive justifications for decisions. To further enhance reliability, rule-based logic is integrated to handle deterministic evaluations for specific, well-defined policy conditions, ensuring consistency in scenarios that require absolute adherence to guidelines.
Below is an example of a recommendation. Please watch the video at the top if you want to see it in action.

Evaluating AutoAuth
Synthetic Data for Case Studies
Why Use Synthetic Data?
Synthetic data avoids privacy issues while still providing realistic and relatable cases. It allows us to demonstrate how AutoAuth operates in real-world medical scenarios without using any patient information.
How Were the Test Cases Built?
To simulate realistic medical cases, we employed a systematic approach driven by clinical insight. Under the guidance of Dr. Pedram, case scenarios were designed to reflect the real-world complexities of prior authorization requests. These test cases are entirely fictional, with no identifiable patient information.
Identification of Key Conditions
- We identified medical conditions that frequently require prior authorization (PA) submissions, such as second and third-line treatments for patients who failed to respond to the standard of care.
Medication Requests
- For each condition, commonly requested medications were selected, along with their associated prior authorization policy criteria.
Case Construction
Using domain expertise and a review of general PA policy guidelines, synthetic cases were developed for each medication. Two versions were created for each case:
Approval Scenario: A scenario designed to demonstrate conditions under which the PA request is expected to be approved based on generalized policy criteria.
Denial Scenario: A second scenario illustrating why a PA request would likely be denied based on clinical facts and policy rules.
Synthetic Data Generation
- Synthetic laboratory and imaging data were generated to support the clinical information in physician notes, as supplemental data is often required in real-world PA requests. No patient data was used, and the synthetic data is fictional.
Evaluation Methodology
Case Design
For each request, two synthetic test cases were created — one designed to meet approval criteria and one designed to trigger a denial.
The case logic is based on general clinical practices and industry-standard PA criteria.
A/B Testing
Each synthetic test case was evaluated using AutoAuth.
The system's decision (Approve, Deny, or Request More Information) was compared against the expected outcome for accuracy.
Explanations provided by AutoAuth were reviewed for alignment with policy logic and clinical reasoning.
Analysis of Performance
The reasoning behind AutoAuth’s decisions was examined to ensure transparency and explainability.
Results were analyzed for any discrepancies, and insights were used to fine-tune system performance.
Evaluation of Results
| Case Diagnosis | Case Medication Request | Expected AutoAuth Decision | Actual AutoAuth Decision and Reasoning | Average Time to Decision |
| Inflammatory Bowel Disease (Crohn’s) | Adalimumab | Approval | “The patient meets all necessary requirements. She is over 6 years old, has tried corticosteroid therapy without improvement, and the medication is prescribed by a pediatric gastroenterologist. Therefore, the prior authorization request should be approved.” | 78 seconds |
| Inflammatory Bowel Disease (Crohn’s) | Adalimumab | Denial | “The PA request is denied. The patient does not meet all the criteria outlined in the policy for initial therapy in Crohn's disease. Specifically, there is no evidence that the patient has tried or is currently taking corticosteroids or another conventional systemic therapy, nor does she meet any alternative criteria under criterion ii. Additionally, the prescribing physician is a pediatrician, not specified as a gastroenterologist, which does not meet criterion iii.” | 84 seconds |
| Lennox-Gastaut Syndrome | Epidiolex | Approval | “The PA request is approved. The patient meets all the necessary criteria outlined in the policy for Lennox-Gastaut Syndrome. The patient is a 2-year-old diagnosed with Lennox-Gastaut Syndrome. The patient has tried or is currently receiving at least two other antiseizure medications (valproic acid, lamotrigine, rufinamide, topiramate). The prescribing physician is a pediatric neurologist.” | 62 seconds |
| Lennox-Gastaut Syndrome | Epidiolex | Denial | “The patient has not demonstrated trial or concomitant use of at least two other anti-seizure medications, and the medication is not prescribed by or in consultation with a neurologist. The PA request is denied.” | 81 seconds |
| Lymphoblastic Leukemia (B-ALL), Philadelphia chromosome-negative | Blinatumomab | Approval | “The PA request is approved. The patient meets all the necessary criteria outlined in the policy for Blincyto use in B-cell precursor acute lymphoblastic leukemia (B-ALL) in remission but positive for minimal residual disease (MRD+).” | 80 seconds |
| Lymphoblastic Leukemia (B-ALL), Philadelphia chromosome-positive | Blinatumomab | Denial | “The patient does not meet all the criteria outlined in the policy. Specifically, for Philadelphia chromosome-positive (Ph+) relapsed or refractory B-cell precursor acute lymphoblastic leukemia (B-ALL), the policy requires that the patient is intolerant or refractory to at least one second-generation or later tyrosine kinase inhibitor (TKI). There is no documentation that the patient has tried a second-generation or later TKI; the patient has only been treated with imatinib, a first-generation TKI. Therefore, the PA request does not meet the necessary criteria for approval.” | 98 seconds |
| Severe Atopic Dermatitis | Dupilumab | Approval | “The PA request meets all the necessary requirements and is approved. The patient has a documented diagnosis of severe atopic dermatitis, has failed to achieve adequate control with two specified classes of topical therapies, is not receiving prohibited concurrent medications, and the prescribing physician is appropriately specialized.” | 77 seconds |
| Severe Atopic Dermatitis | Dupilumab | Denial | “The PA request does not meet all the necessary criteria outlined in the policy for atopic dermatitis. Specifically, the patient has a history of failure with only one class of topical therapy, whereas the policy requires a history of failure, contraindication, or intolerance to two specified classes of topical therapies.” | 76 seconds |
| High-grade Osteosarcoma | Everolimus | Approval | “The PA request for Afinitor (everolimus) is approved. The patient meets all the necessary criteria outlined in the policy for the use of Afinitor in combination with Nexavar (sorafenib) for metastatic osteosarcoma as second-line therapy.” | 71 seconds |
| High-grade Osteosarcoma | Everolimus | Denial | “The PA request for Afinitor (everolimus) is denied because it does not meet all the necessary criteria outlined in the policy for the treatment of osteosarcoma. Specifically, the policy requires that Afinitor be used in combination with Nexavar (sorafenib) for this indication, and there is no evidence provided that Nexavar is part of the treatment plan.” | 81 seconds |
Performance Metrics:
Accuracy: % of AutoAuth decisions that match human decisions.
Time Savings: Average time reduction from manual PA to AutoAuth.
Key Findings:
100% accuracy in 10 synthetic cases.
AutoAuth reduces processing time from hours to minutes, with an average overall processing time of under two minutes (79 seconds)
Transparent and detailed reasoning provided for every decision with direct reference to policy text and provided clinical data
The Value Of Time
Let’s take Contoso, a global leader in the insurance industry (Payor), as an example to illustrate this concept. PA Specialists were drowning in repetitive tasks, processing one case at a time while costs kept piling up. The above results clearly demonstrated how AI could drive staggering productivity improvements — but for this example, let’s take a highly conservative approach. Let’s assume Contoso improved productivity by a modest 2x.

How Does That Translate Into Savings?
Before AI Adoption - Contoso’s specialists managed PA workflows the old-fashioned way. With 145 specialists working 8 hours a day for 22 days a month, they could process 1 case per hour, handling 25,520 cases per month. At a cost of $60 per case, this totaled $1.5M per month — a significant operational expense.
After AI Adoption - By integrating an AI-powered framework into their workflows, productivity at Contoso doubled. Specialists began processing 2 cases per hour, scaling operations to 51,040 cases per month. With the cost per case dropping to $30, they achieved the same workload for half the cost.
The Impact:
This shift didn’t just streamline operations; it saved Contoso a staggering $1.5M per month, totaling $18M in annual savings. Specialists were no longer bogged down by repetitive tasks, instead focusing on higher-value decision-making while the AI handled the grunt work.
Key Take Aways
This AI transformative shift represents a staggering $18M in annual savings for Contoso — time reclaimed, errors reduced, and decision-making amplified. By accelerating human decision-making, AutoAuth doesn't just optimize workflow; it redefines what "time well spent" means in healthcare.
Efficiency by AI. Decisions by You. That's the value of time, doubled.
References
1. American Medical Association, "Prior Authorization Research Reports" (https://www.ama-assn.org/practice-management/prior-authorization/prior-authorization-research-reports)
2. Sagility Health, "Transformative AI to Revamp Prior Authorizations" (https://sagilityhealth.com/news/transformative-ai-to-revamp-prior-authorizations/)
3. McKinsey, "AI Ushers in Next-Gen Prior Authorization in Healthcare" (https://www.mckinsey.com/industries/healthcare/our-insights/ai-ushers-in-next-gen-prior-authorization-in-healthcare)
4. Centers for Medicare and Medicaid Services, “CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F)”
5. Council for Affordable Quality Healthcare (CAQH) Insights, “2023 CAQH Index Report”
(https://www.caqh.org/hubfs/43908627/drupal/2024-01/2023_CAQH_Index_Report.pdf)
6. Cigna Healthcare, “Prior Authorization Policy Inflammatory Conditions - Adalimumab”
7. Cigna Healthcare, “Epidiolex Prior Authorization Policy”
8. Envolve Pharmacy Solutions, “Clinical Policy: Blinatumomab (Blincyto)”
9. United Healthcare, “Dupilumab Prior Authorization”
10. United Healthcare, “Everolimus Prior Authorization”
11. American Medical Association, “Fixing prior auth: First, speed up payers’ response times”
12. American Medical Association, “2023 AMA prior authorization survey”
(https://www.ama-assn.org/system/files/prior-authorization-survey.pdf)